
A Mechanism-Aware Decision Infrastructure for Stroke
A Mechanism-Aware Decision Infrastructure for Stroke
We build systems that understand why ischemic stroke happens — not just that it happened — and use that insight to guide precise, evidence-based care decisions.
BASE™ is a 1,700-patient prospective transcriptomic stroke cohort that anchors our mechanism-aware decision infrastructure and was built for clinical deployment.
BASE™ links acute neurovascular biology to actionable secondary prevention before mechanism is traditionally known.
Our first clinical focus is secondary stroke prevention — delivering earlier biological clarity to connect the right patient, right time, and right therapy.
The first clinical application
Secondary Prevention Limited Before Mechanism Is Known
Secondary Prevention Limited Before Mechanism Is Known
695,000
Ischemic strokes annually (U.S.)
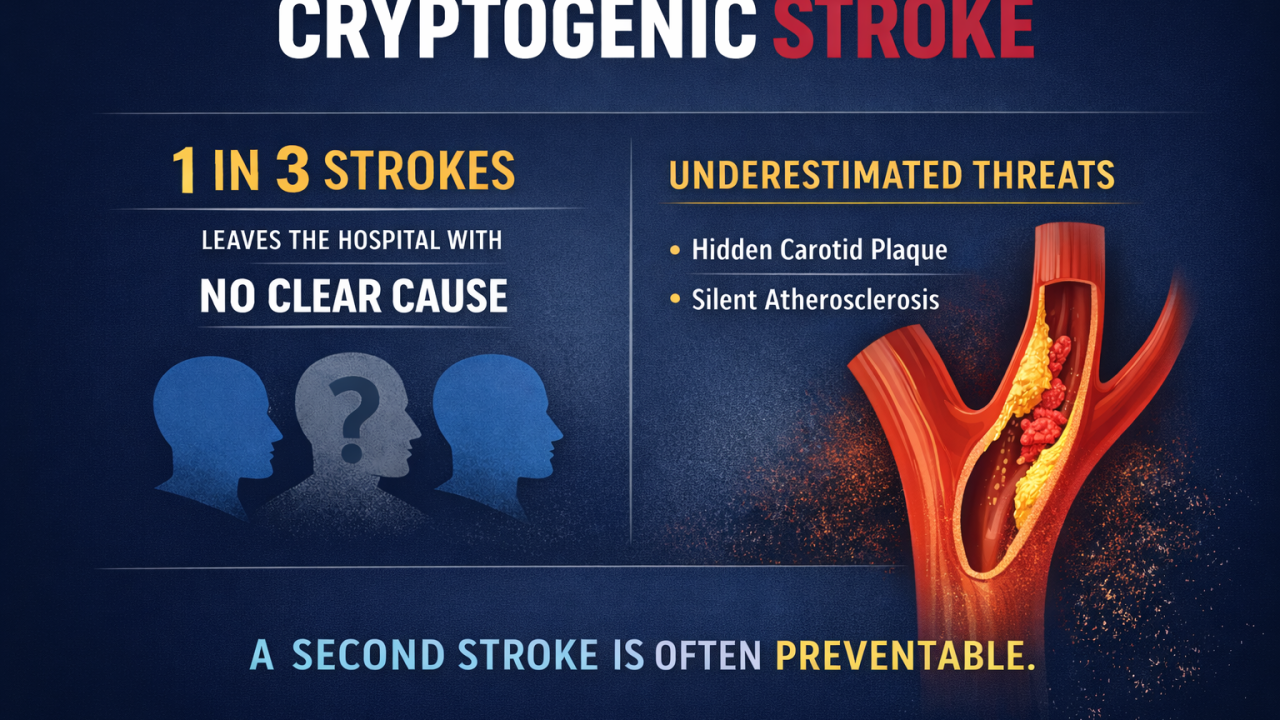
30-40%
Leave the hospital classified as cryptogenic
~185,000
Recurrent strokes annually, with highest risk highest at 30 days and 1 year
“Cryptogenic” does not mean there was no cause. It means the biological driver was not identified in time to guide mechanism-specific prevention.
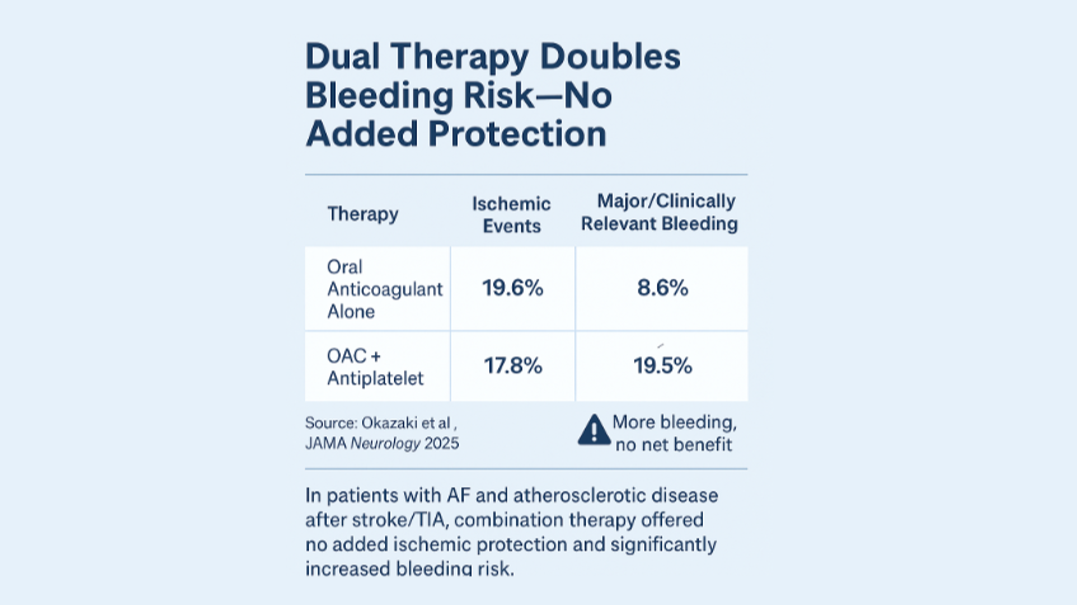
Therapeutic options are expanding for secondary prevention — DAPT, FXIa inhibitors, and beyond — but precision requires mechanism. The problem is not lack of therapy. It is lack of biological clarity at the time decisions are made. Secondary prevention is increasingly powerful — but only as precise as the mechanism it reflects.
Mechanism determines which therapy, when, and for whom.
Mechanism-based care prevents avoidable strokes and hospitalizations. Without earlier mechanism identification, secondary prevention remains reactive rather than preventive.
Therapeutic options are expanding for secondary prevention — DAPT, FXIa inhibitors, and beyond — but precision requires mechanism. The problem is not lack of therapy. It is lack of biological clarity at the time decisions are made. Secondary prevention is increasingly powerful — but only as precise as the mechanism it reflects.
Mechanism determines which therapy, when, and for whom.
Mechanism-based care prevents avoidable strokes and hospitalizations. Without earlier mechanism identification, secondary prevention remains reactive rather than preventive.

Our Foundation
BASE: The Mechanism Engine
BASE: The Mechanism Engine
BASE originated as a prospective, real-world suspected stroke cohort enrolling consecutive patients presenting with acute neurologic symptoms across 20+ hospital systems. The cohort includes ischemic stroke, transient ischemic attack (TIA), and transient neurologic events (TNE), reflecting how stroke presents in practice — before full diagnostic certainty.
Cohort Foundation:
- 1,700 patients
- 5,000+ acute blood samples
- Prospectively adjudicated 90-day outcomes
- Longitudinal design supported by $25M in funding
- NCT02014896
Acute-window blood collection enables time-resolved transcriptomic analysis linked to adjudicated mechanism and longitudinal outcomes.
The prospective, multi-center design and adjudicated outcomes create a biological foundation that is difficult to replicate and engineered for deployment.
BASE quantifies stroke mechanism earlier than traditional workups converge — transforming acute biology into actionable signal.
The prospective, multi-center design and adjudicated outcomes create a biological foundation that is difficult to replicate and engineered for deployment.
BASE quantifies stroke mechanism earlier than traditional workups converge — transforming acute biology into actionable signal.
The Architecture
From Cohort to Infrastructure
From Cohort to Infrastructure
BASE operates as a layered decision architecture anchored to a single adjudicated biological core and deployed across clinical and translational domains. The architecture is structured for integration across diagnostic platforms, imaging ecosystems, therapeutic portfolios, and risk-bearing health systems.
Multiple integration pathways. One mechanism engine.
Multiple integration pathways. One mechanism engine.
BASE™
Mechanism Engine
Time-resolved transcriptomic signatures quantifying stroke subtype and underlying mechanism in the acute window.
ISCDx™
Clinical Stratification
Mechanism-aware classification deployed within hospital workflows.
The first expression of this infrastructure was ISCDx™ — a mechanism-identification layer demonstrating that acute biology can inform secondary prevention decisions and serve as a clinical learning vehicle of the BASE engine.
The first expression of this infrastructure was ISCDx™ — a mechanism-identification layer demonstrating that acute biology can inform secondary prevention decisions and serve as a clinical learning vehicle of the BASE engine.
STRIDE™
Workflow Compression
Decision support prioritizing escalation, monitoring, and secondary prevention within existing care pathways.
Neuroformer™
AI Modeling
Scalable predictive models trained on longitudinal biologic and adjudicated clinical data, embedded within clinical workflow rather than developed in isolation.
BASE Explorer™
Data & Biopharma Layer
Real-world biologic enrichment, hypothesis generation, and translational licensing.
Multi-Modal Integration
Built to Enhance Existing Stroke Iinfrastructure
Built to Enhance Existing Stroke Iinfrastructure
Imaging defines the presence of stroke
Therapeutics expand treatment options.
Monitoring tools refine long-term detection.
Digital platforms coordinate care pathways.
BASE infrastructure is built to integrate across imaging, diagnostic, therapeutic, monitoring, and digital health platforms — serving as a biological intelligence layer within broader neurovascular ecosystems.

Real-World Impact
Workflow-Native Deployment
Workflow-Native Deployment
Blood-based mechanistic insight integrated directly into a community hospital stroke workflow.
Prospective Pilot (VAC approved)
- 30% management modification rate
- Estimated ~$1,750 per-patient cost offset
- Reduced repeat procedures
- Improved escalation decisions
- Increased clinical confidence and patient clarity
Evaluation occurred within real-time care delivery, not retrospective review.
The impact was not diagnostic replacement, but decision refinement within existing care pathways.
The deployment model is structured to integrate within imaging, monitoring, and therapeutic pathways without disrupting established care.
A care pathway should not require months of uncertainty.
The impact was not diagnostic replacement, but decision refinement within existing care pathways.
The deployment model is structured to integrate within imaging, monitoring, and therapeutic pathways without disrupting established care.
A care pathway should not require months of uncertainty.
.jpg)
The BASE Advantage
Why This Infrastructure Is Distinct
Why This Infrastructure Is Distinct
BASE is not a retrospective data aggregation or synthetic cohort. It is a prospective, multi-center, adjudicated biological foundation embedded within real-world stroke workflow.
The prospective structure of BASE enables model development grounded in adjudicated biological truth rather than synthetic training data. Its structure reflects years of coordinated enrollment, acute-window biospecimen capture, longitudinal follow-up, and cross-system variability.
The prospective structure of BASE enables model development grounded in adjudicated biological truth rather than synthetic training data. Its structure reflects years of coordinated enrollment, acute-window biospecimen capture, longitudinal follow-up, and cross-system variability.
Cohort Foundation:
- Prospective rather than retrospective
- Acute and time-resolved rather than archival
- Linked to adjudicated outcomes rather than billing codes
- Embedded in real-world workflow across 20+ health systems
- Supported by additional banked samples and deployable architecture
The infrastructure supports advanced modeling and machine learning grounded in prospective biological data rather than retrospective abstraction.
This is not a downloadable dataset. It is a translational engine designed for clinical integration.
Reproducing this infrastructure would require years of prospective enrollment, acute biospecimen capture, adjudication, and cross-system integration. The result is infrastructure designed not as a standalone product, but as a strategic layer within broader neurovascular ecosystems.
This is not a downloadable dataset. It is a translational engine designed for clinical integration.
Reproducing this infrastructure would require years of prospective enrollment, acute biospecimen capture, adjudication, and cross-system integration. The result is infrastructure designed not as a standalone product, but as a strategic layer within broader neurovascular ecosystems.
Our Articles
Our Articles
From decoding the molecular signatures of atherosclerosis to critiquing the limitations of traditional AI, our writing explores how a deeper understanding of stroke biology is reshaping the care pathways of the future.
The Next Era of Stroke Care Will Be Built on Mechanism
The Next Era of Stroke Care Will Be Built on Mechanism
Mechanism aware infrastructure linked to real-world workflow is no longer theoretical. It is deployable, scalable, and inherently difficult to replicate. BASE serves as the biological core for a new generation of precision stroke care systems — aligned with clinical excellence, therapeutic innovation, and value-based outcomes. For organizations advancing neurovascular strategy, therapeutic development, health system transformation, or risk-aligned care models, we welcome confidential strategic engagement.
I founded Ischemia Care and led the BASE clinical trial, which generated one of the largest deeply annotated multi-omic datasets in stroke. Through that work we commercialized one of the first blood tests for stroke to be used clinically, giving us a unique window into how molecular signals translate into real clinical decision making.
What became clear over time is that the real asset isn’t just a single diagnostic, but the biological infrastructure behind the dataset.
We’re now expanding that work through a new division called BASE Bio, which focuses on using AI and transcriptomic data to build mechanism-aware models of neurovascular disease. The goal is to move beyond standalone diagnostic tests and create a platform that connects biology, clinical workflows, and decision infrastructure.
In parallel, I stay very active in the global innovation ecosystem through programs like MedTech Innovator and several international accelerators. That vantage point keeps me close to emerging technologies while continuing to advance the biological platform we built through BASE.
What became clear over time is that the real asset isn’t just a single diagnostic, but the biological infrastructure behind the dataset.
We’re now expanding that work through a new division called BASE Bio, which focuses on using AI and transcriptomic data to build mechanism-aware models of neurovascular disease. The goal is to move beyond standalone diagnostic tests and create a platform that connects biology, clinical workflows, and decision infrastructure.
In parallel, I stay very active in the global innovation ecosystem through programs like MedTech Innovator and several international accelerators. That vantage point keeps me close to emerging technologies while continuing to advance the biological platform we built through BASE.

Jeff June
Founder, Board Member