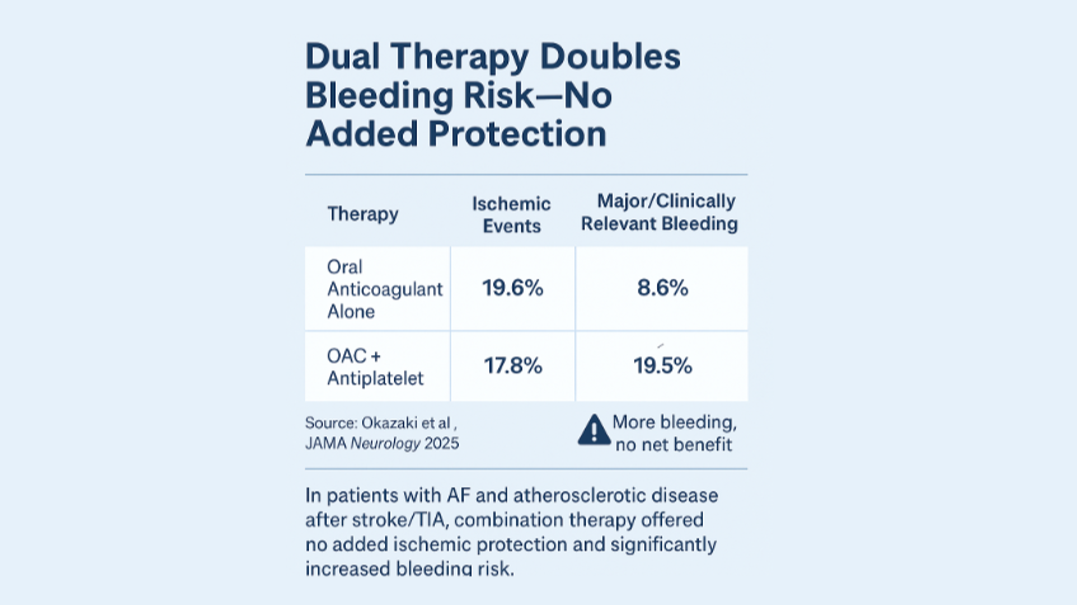
A new JAMA Neurology study caught my attention this week: patients with both #atrialfibrillation (#AF) and #atherosclerotic disease — two of the most common contributors to stroke — were randomized to either #anticoagulation alone or anticoagulation plus an #antiplatelet drug. The result? No improvement in preventing future ischemic events, but double the bleeding risk for those on combination therapy.
With respect to care pathways to prevent recurrent stroke, citing information in this article, it reflects how uncertainty about why a stroke occurred can ripple through treatment decisions, leading to excess medications, bleeding events, and avoidable hospitalizations.
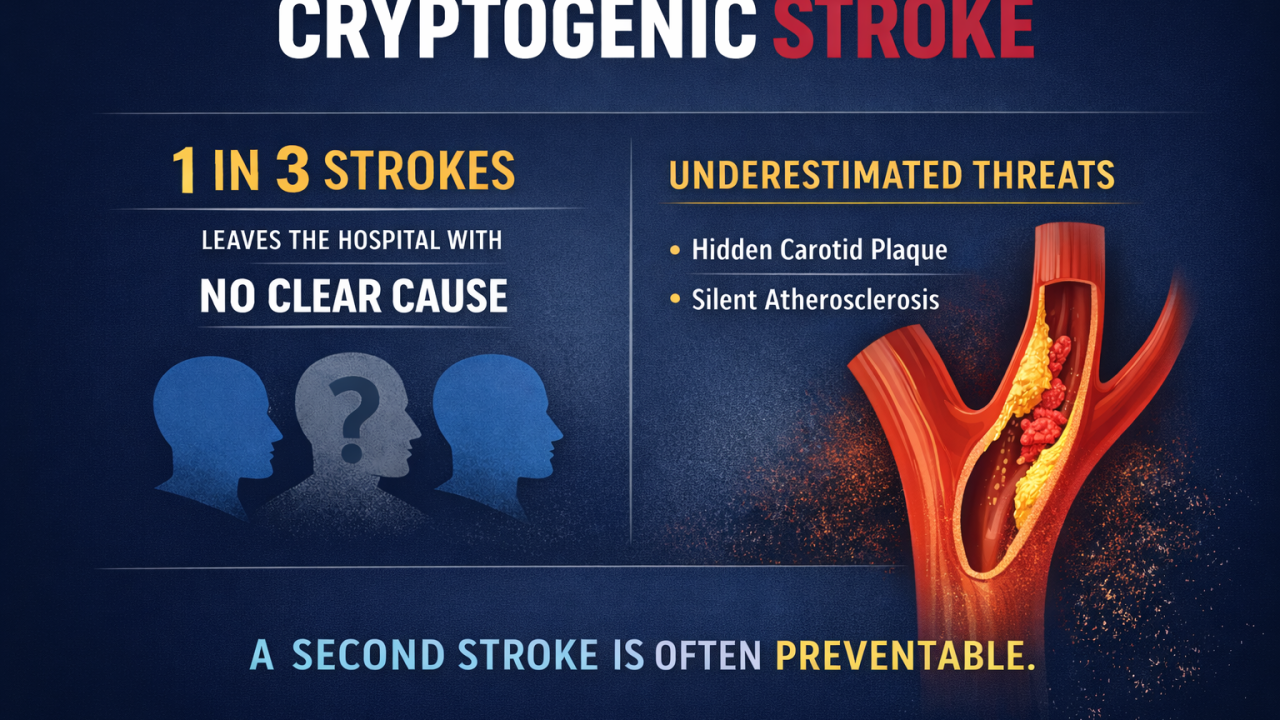
Precision Starts with Etiology
In stroke, mechanism isn’t academic — it drives therapeutic care. An embolic stroke from AF behaves very differently than one driven by plaque rupture, small vessel disease, or paradoxical embolism. However, care pathways may treat these subtypes the same way, defaulting to broad coverage. Let me be clear on this point, we live in the golden age of stroke care where state of the art intervention provides incredible outcomes for the index event, meaning the stroke that just happened, but what about the next stroke if we don't know what cause the first?
That reflex to treat broadly may make sense emotionally — but physiologically, it can be increase risk. Getting the cause right determines whether to anticoagulate, whether to add antiplatelet therapy, and how to monitor for recurrence. When the cause is uncertain, the article suggests to system leans toward over-treatment.
A Smarter Future for Stroke and Cardiovascular Care
I’ve spent much of my career focused on this question — founding a company to decode stroke biology and mentoring startups working at the intersection of diagnostics, AI, and cardiovascular health. Across all of them, one principle holds true:
When we understand cause, we can personalize care — not generalize it.
Emerging tools now let us classify stroke by its molecular, electrical, and anatomical signatures rather than by exclusion. That potentially means fewer “#cryptogenic” strokes, faster decisions, and better alignment between clinician intent and biological reality.
Imagine a near future where the post-stroke care team doesn’t just ask “what happened?” but “why did it happen, and how does that change what we do next?”
Bridging the Gap
This week’s trial reinforces that more drugs aren’t always more protection — sometimes, they’re more harm. But it also underscores a deeper need: decision support rooted in #etiology, not habit.
Whether through #AI-assisted imaging, #gen expression profiling, or integrated data pipelines, our goal should be to turn uncertainty into clarity — so treatment can finally be guided by mechanism, not guesswork.
That’s the kind of translational work I’m proud to see gaining momentum across the stroke and cardiovascular community — from the startups I mentor to the innovators reshaping how we define and manage disease.
Closing Thought
Stroke care is about reacting to an event and immediacy of care. It’s also about a longer term care pathway for anticipating patterns, recognizing causes, and building systems that prevent recurrence without unnecessary harm. Thank you for reading this piece!
Okazaki S, Tanaka K, Yazawa Y, et al; ATIS-NVAF Trial Investigators.Optimal Antithrombotics for Ischemic Stroke and Concurrent Atrial Fibrillation and Atherosclerosis: A Randomized Clinical Trial.JAMA Neurology. Published online October 6, 2025.doi:10.1001/jamaneurol.2025.3662